
Search
- Page Path
- HOME > Search
Review Article
- Diabetes, Obesity and Metabolism
- Renal Protection of Mineralocorticoid Receptor Antagonist, Finerenone, in Diabetic Kidney Disease
- Dong-Lim Kim, Seung-Eun Lee, Nan Hee Kim
- Endocrinol Metab. 2023;38(1):43-55. Published online February 27, 2023
- DOI: https://doi.org/10.3803/EnM.2022.1629
- 5,707 View
- 773 Download
- 5 Web of Science
- 7 Crossref
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader  ePub
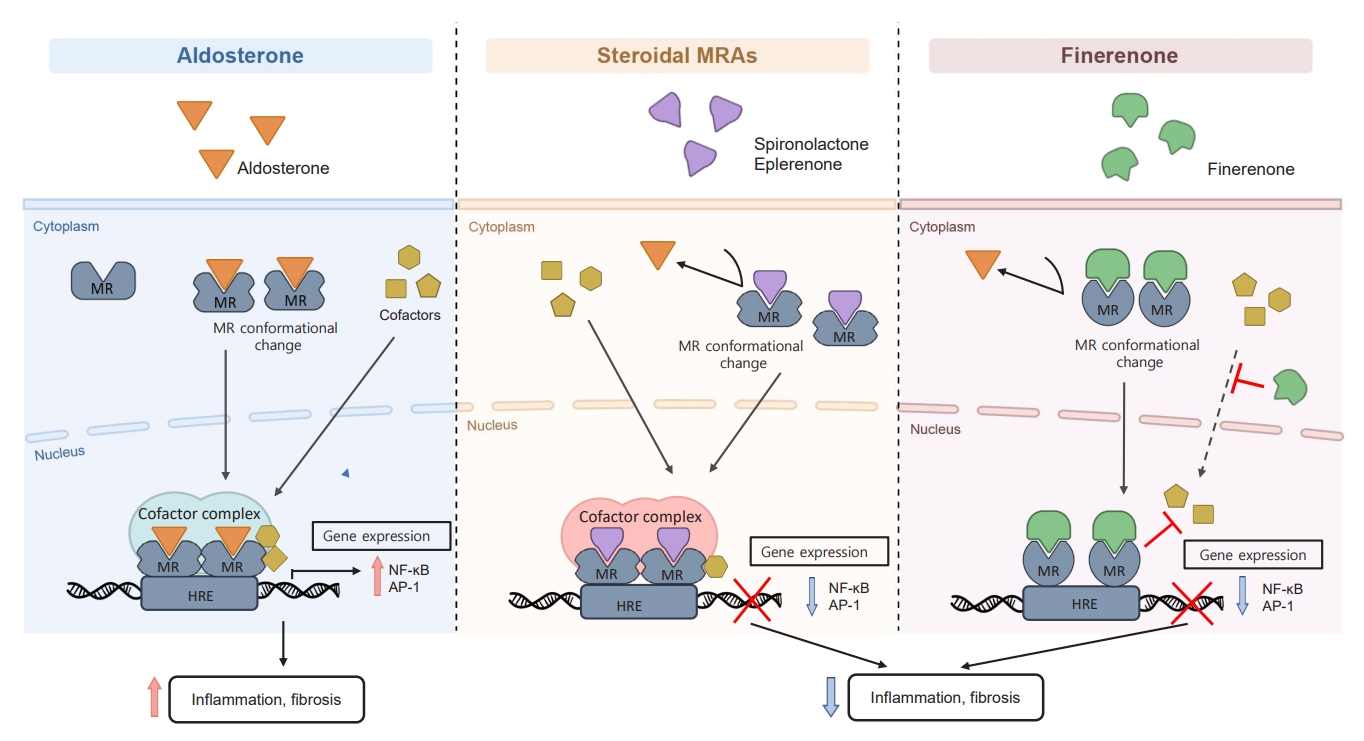
ePub - Chronic kidney disease (CKD) is the most common cause of end-stage renal disease in patients with type 2 diabetes mellitus (T2DM). CKD increases the risk of cardiovascular diseases; therefore, its prevention and treatment are important. The prevention of diabetic kidney disease (DKD) can be achieved through intensive glycemic control and blood pressure management. Additionally, DKD treatment aims to reduce albuminuria and improve kidney function. In patients with T2DM, renin-angiotensin-aldosterone system inhibitors, sodium glucose cotransporter 2 inhibitors, and glucagon-like peptide-1 receptor agonists can delay the progression of DKD. Hence, there is a need for novel treatments that can effectively suppress DKD progression. Finerenone is a first-in-class nonsteroidal mineralocorticoid receptor antagonist with clinically proven efficacy in improving albuminuria, estimated glomerular filtration rate, and risk of cardiovascular events in early and advanced DKD. Therefore, finerenone is a promising treatment option to delay DKD progression. This article reviews the mechanism of renal effects and major clinical outcomes of finerenone in DKD.
-
Citations
Citations to this article as recorded by
- Neue Antihypertensiva im Renin-Angiotensin-Aldosteron-System
Markus van der Giet
CardioVasc.2024; 24(1): 33. CrossRef -
Chicoric acid
advanced PAQR3 ubiquitination to ameliorate ferroptosis in diabetes nephropathy through the relieving of the interaction between PAQR3 and P110α pathway
Weiwei Zhang, Yong Liu, Jiajun Zhou, Teng Qiu, Haitang Xie, Zhichen Pu
Clinical and Experimental Hypertension.2024;[Epub] CrossRef - Endothelial CXCR2 deficiency attenuates renal inflammation and glycocalyx shedding through NF-κB signaling in diabetic kidney disease
Siyuan Cui, Xin Chen, Jiayu Li, Wei Wang, Deqi Meng, Shenglong Zhu, Shiwei Shen
Cell Communication and Signaling.2024;[Epub] CrossRef - Molecular Targets of Novel Therapeutics for Diabetic Kidney Disease: A New Era of Nephroprotection
Alessio Mazzieri, Francesca Porcellati, Francesca Timio, Gianpaolo Reboldi
International Journal of Molecular Sciences.2024; 25(7): 3969. CrossRef - Epigenetic modification in diabetic kidney disease
Zhe Liu, Jiahui Liu, Wanning Wang, Xingna An, Ling Luo, Dehai Yu, Weixia Sun
Frontiers in Endocrinology.2023;[Epub] CrossRef - Novel Approaches in Chronic Renal Failure without Renal Replacement Therapy: A Review
Sandra Martínez-Hernández, Martín Muñoz-Ortega, Manuel Ávila-Blanco, Mariana Medina-Pizaño, Javier Ventura-Juárez
Biomedicines.2023; 11(10): 2828. CrossRef - Finerenone and other future therapeutic options for Alport syndrome
Helen Pearce, Holly Mabillard
Journal of Rare Diseases.2023;[Epub] CrossRef
- Neue Antihypertensiva im Renin-Angiotensin-Aldosteron-System

Original Articles
- Clinical Study
- Impaired Cortisol and Growth Hormone Counterregulatory Responses among Severe Hypoglycemic Patients with Type 2 Diabetes Mellitus
- Young A Rhyu, Ju-Young Jang, Sooyoun Park, Jee Hyun An, Dong-Lim Kim, Suk Kyeong Kim, Kee-Ho Song
- Endocrinol Metab. 2019;34(2):187-194. Published online June 24, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.2.187
- 5,035 View
- 75 Download
- 10 Web of Science
- 12 Crossref
-
Abstract
PDFPubReader ePub
Background Elevated levels of cortisol and growth hormone are critical counterregulatory responses to severe hypoglycemia. However, the proportion and clinical characteristics of patients with type 2 diabetes mellitus (DM) who fail to show appropriate cortisol and/or growth hormone secretion in response to severe hypoglycemia have not been investigated.
Methods We measured plasma cortisol and growth hormone levels in type 2 DM patients with severe hypoglycemia who visited the emergency department between 2006 and 2015.
Results Of 112 hypoglycemic patients, 23 (20.5%) had an impaired cortisol response (<18 µg/dL) and 82 patients (73.2%) had an impaired growth hormone response (<5 ng/mL). Nineteen patients (17.0%) had impaired responses to both cortisol and growth hormone. The patients with impaired responses of cortisol, growth hormone, and both hormones were significantly older and more likely to be female, and had higher admission rates, lower growth hormone levels, and lower adrenocorticotropic hormone levels than the patients with a normal hormonal response. Multivariate logistic regression analysis indicated that an impaired growth hormone response was significantly associated with advanced age, shorter DM duration, a higher admission rate, and a higher body mass index (BMI). An impaired cortisol response was significantly associated with growth hormone levels. Patients with an impaired growth hormone response had higher admission rates than patients with a normal response.
Conclusion A considerable number of type 2 DM patients had impaired cortisol and/or growth hormone responses to severe hypoglycemia. Advanced age, shorter DM duration, and higher BMI were independently associated with an abnormal growth hormone response.
-
Citations
Citations to this article as recorded by- The deleterious effects of sofosbuvir and ribavirin (antiviral drugs against hepatitis C virus) on different body systems in male albino rats regarding reproductive, hematological, biochemical, hepatic, and renal profiles and histopathological changes
Rana A. Ali, Eatemad A. Awadalla, Yahia A. Amin, Samer S. Fouad, Maha Abd-El Baki Ahmed, Mohammed H. Hassan, Emaad Abdel-Kahaar, Rehab H. Abdel-Aziz
Scientific Reports.2024;[Epub] CrossRef - Prediabetes and mild hepatosteatosis are associated with blunted cortisol response to glucagon but not to growth hormone
Ozlem Deveci, Zuleyha Karaca, Fatih Tanriverdi, Kamil Deveci, Aysa Hacioglu, Kursad Unluhizarci, Fahrettin Kelestimur
Annales d'Endocrinologie.2023; 84(2): 254. CrossRef - Evaluación del cortisol plasmático durante el test de ayuno en pacientes con síndrome hipoglucémico por hiperinsulinismo endógeno. Experiencia de 15 años
María Eugenia Gullace, María Victoria Ortuño, Teresa Mabel Canteros, Belén Bosco, Cintia Rodriguez, Javier Giunta, Lucas Costa, Andrea Kozak, Valeria de Miguel, Luis Grosembacher
Endocrinología, Diabetes y Nutrición.2023; 70(10): 634. CrossRef - Evaluation of plasma cortisol during fasting test in patients with endogenous hyperinsulinemic hypoglycemia. Fifteen years experience
María Eugenia Gullace, María Victoria Ortuño, Teresa Mabel Canteros, Belén Bosco, Cintia Rodriguez, Javier Giunta, Lucas Costa, Andrea Kozak, Valeria de Miguel, Luis Grosembacher
Endocrinología, Diabetes y Nutrición (English ed.).2023; 70(10): 634. CrossRef - Cerebrospinal fluid levels of hypothalamic-pituitary-adrenal axis hormones in MCI and dementia due to Alzheimer’s disease: a systematic review
Felipe Duarte-Zambrano, Jorge A. Barrero, Ismena Mockus
Dementia & Neuropsychologia.2023;[Epub] CrossRef - PTEN Deletion in Adult Mice Induces Hypoinsulinemia With Concomitant Low Glucose Levels
Maria Crespo-Masip, Aurora Pérez-Gómez, Carla Guzmán, Sandra Rayego, Nuria Doladé, Alicia García-Carrasco, Ramiro Jover, José Manuel Valdivielso
Frontiers in Endocrinology.2022;[Epub] CrossRef - Beta Blockers can Mask not only Hypoglycemia but also Hypotension
Goran Koracevic, Sladjana Micic, Milovan Stojanovic, Radmila Velickovic Radovanovic, Milan Pavlovic, Tomislav Kostic, Dragan Djordjevic, Nebojsa Antonijevic, Maja Koracevic, Vesna Atanaskovic, Sonja Dakic
Current Pharmaceutical Design.2022; 28(20): 1660. CrossRef - Atherosclerosis Risk Factors in Patients with Reactive Hypoglycemia
Małgorzata Landowska, Agata Żebrowska, Konrad Fajer, Patrycja Adamek, Aleksandra Kruk, Bernadetta Kałuża, Edward Franek
Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2022; Volume 15: 3133. CrossRef - Depression with Comorbid Diabetes: What Evidence Exists for Treatments Using Traditional Chinese Medicine and Natural Products?
Yanting Lu, Tao An, Hu Tian, Xueqin Gao, Furong Wang, Shijun Wang, Ke Ma
Frontiers in Pharmacology.2021;[Epub] CrossRef - Hepatocyte-specific glucose-6-phosphatase deficiency disturbs platelet aggregation and decreases blood monocytes upon fasting-induced hypoglycemia
Anouk M. La Rose, Venetia Bazioti, Joanne A. Hoogerland, Arthur F. Svendsen, Anouk G. Groenen, Martijn van Faassen, Martijn G.S. Rutten, Niels J. Kloosterhuis, Bertien Dethmers-Ausema, J. Hendrik Nijland, Gilles Mithieux, Fabienne Rajas, Folkert Kuipers,
Molecular Metabolism.2021; 53: 101265. CrossRef - Effects of tofogliflozin on adrenocorticotropic hormone, renin and aldosterone, and cortisol levels in elderly patients with diabetes mellitus
Toshihiro Higashikawa, Tomohiko Ito, Takurou Mizuno, Keiichirou Ishigami, Kengo Kuroki, Naoto Maekawa, Daisuke Usuda, Takuro Morita, Kazu Hamada, Susumu Takagi, Kento Takeshima, Shinya Yamada, Ryusho Sangen, Toshihide Izumida, Hideyuki Mori, Jun Kiyosawa,
Medicine.2021; 100(45): e27638. CrossRef - Stress, glucocorticoid signaling pathway, and metabolic disorders
Roldan M. de Guia
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2020; 14(5): 1273. CrossRef
- The deleterious effects of sofosbuvir and ribavirin (antiviral drugs against hepatitis C virus) on different body systems in male albino rats regarding reproductive, hematological, biochemical, hepatic, and renal profiles and histopathological changes
- Effects of Vildagliptin or Pioglitazone on Glycemic Variability and Oxidative Stress in Patients with Type 2 Diabetes Inadequately Controlled with Metformin Monotherapy: A 16-Week, Randomised, Open Label, Pilot Study
- Nam Hoon Kim, Dong-Lim Kim, Kyeong Jin Kim, Nan Hee Kim, Kyung Mook Choi, Sei Hyun Baik, Sin Gon Kim
- Endocrinol Metab. 2017;32(2):241-247. Published online June 23, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.2.241
- 4,650 View
- 94 Download
- 23 Web of Science
- 23 Crossref
-
Abstract
PDFPubReader
Background Glycemic variability is associated with the development of diabetic complications through the activation of oxidative stress. This study aimed to evaluate the effects of a dipeptidyl peptidase 4 inhibitor, vildagliptin, or a thiazolidinedione, pioglitazone, on glycemic variability and oxidative stress in patients with type 2 diabetes.
Methods In this open label, randomised, active-controlled, pilot trial, individuals who were inadequately controlled with metformin monotherapy were assigned to either vildagliptin (50 mg twice daily,
n =17) or pioglitazone (15 mg once daily,n =14) treatment groups for 16 weeks. Glycemic variability was assessed by calculating the mean amplitude of glycemic excursions (MAGE), which was obtained from continuous glucose monitoring. Urinary 8-iso prostaglandin F2α, serum oxidised low density lipoprotein, and high-sensitivity C-reactive protein were used as markers of oxidative stress or inflammation.Results Both vildagliptin and pioglitazone significantly reduced glycated hemoglobin and mean plasma glucose levels during the 16-week treatment. Vildagliptin also significantly reduced the MAGE (from 93.8±38.0 to 70.8±19.2 mg/dL,
P =0.046), and mean standard deviation of 24 hours glucose (from 38±17.3 to 27.7±6.9,P =0.026); however, pioglitazone did not, although the magnitude of decline was similar in both groups. Markers of oxidative stress or inflammation including urinary 8-iso prostaglandin F2α did not change after treatment in both groups.Conclusion In this 16-week treatment trial, vildagliptin, but not pioglitazone, reduced glycemic variability in individuals with type 2 diabetes who was inadequately controlled with metformin monotherapy, although a reduction of oxidative stress markers was not observed.
-
Citations
Citations to this article as recorded by- What is Glycaemic Variability and which Pharmacological Treatment Options are Effective? A Narrative Review
Juan Miguel Huertas Cañas, Maria Alejandra Gomez Gutierrez, Andres Bedoya Ossa
European Endocrinology.2023; 19(2): 4. CrossRef - Glycemic Variability, Glycated Hemoglobin, and Cardiovascular Complications: Still a Dilemma in Clinical Practice
Antonio Ceriello, Ali A. Rizvi, Manfredi Rizzo
Advances in Therapy.2022; 39(1): 1. CrossRef - Contrasting Three Non-hypoglycemic Antidiabetic Drug Effects on Glycemic Control in Newly Diagnosed Type II Diabetes Mellitus: An Experimental Study
Abdulhamza Hmood, Mohammed Almasoody, Hameed Hussein Al-Jameel
Open Access Macedonian Journal of Medical Sciences.2022; 10(B): 506. CrossRef - Hypoglycemic agents and glycemic variability in individuals with type 2 diabetes: A systematic review and network meta-analysis
SuA Oh, Sujata Purja, Hocheol Shin, Minji Kim, Eunyoung Kim
Diabetes and Vascular Disease Research.2022; 19(3): 147916412211068. CrossRef - Influence of dipeptidyl peptidase-4 inhibitors on glycemic variability in patients with type 2 diabetes: A meta-analysis of randomized controlled trials
Shangyu Chai, Ruya Zhang, Ye Zhang, Richard David Carr, Yiman Zheng, Swapnil Rajpathak, Miao Yu
Frontiers in Endocrinology.2022;[Epub] CrossRef - Comparison of Efficacy of Glimepiride, Alogliptin, and Alogliptin-Pioglitazone as the Initial Periods of Therapy in Patients with Poorly Controlled Type 2 Diabetes Mellitus: An Open-Label, Multicenter, Randomized, Controlled Study
Hae Jin Kim, In Kyung Jeong, Kyu Yeon Hur, Soo-Kyung Kim, Jung Hyun Noh, Sung Wan Chun, Eun Seok Kang, Eun-Jung Rhee, Sung Hee Choi
Diabetes & Metabolism Journal.2022; 46(5): 689. CrossRef - Effect of low dose allopurinol on glycemic control and glycemic variability in patients with type 2 diabetes mellitus: A cross-sectional study
Manal M. Alem
Heliyon.2022; 8(11): e11549. CrossRef - Effect of hydroxychloroquine on glycemic variability in type 2 diabetes patients uncontrolled on glimepiride and metformin therapy
Rajesh Rajput, Suyasha Saini, Siddhant Rajput, Parankush Upadhyay
Indian Journal of Endocrinology and Metabolism.2022; 26(6): 537. CrossRef - Effect of Dapagliflozin as an Add-on Therapy to Insulin on the Glycemic Variability in Subjects with Type 2 Diabetes Mellitus (DIVE): A Multicenter, Placebo-Controlled, Double-Blind, Randomized Study
Seung-Hwan Lee, Kyung-Wan Min, Byung-Wan Lee, In-Kyung Jeong, Soon-Jib Yoo, Hyuk-Sang Kwon, Yoon-Hee Choi, Kun-Ho Yoon
Diabetes & Metabolism Journal.2021; 45(3): 339. CrossRef - Comprehensive elaboration of glycemic variability in diabetic macrovascular and microvascular complications
Bao Sun, Zhiying Luo, Jiecan Zhou
Cardiovascular Diabetology.2021;[Epub] CrossRef - CGMS and Glycemic Variability, Relevance in Clinical Research to Evaluate Interventions in T2D, a Literature Review
Anne-Esther Breyton, Stéphanie Lambert-Porcheron, Martine Laville, Sophie Vinoy, Julie-Anne Nazare
Frontiers in Endocrinology.2021;[Epub] CrossRef - Efficacy and safety profile of sitagliptin, vildagliptin, and metformin in newly diagnosed type 2 diabetic subjects
Sahar Hossam Elhini, Amal K. Hussien, Ahmed Abd Elsamie Omran, Asmaa A. Elsayed, Haitham saeed
Clinical and Experimental Pharmacology and Physiology.2021; 48(12): 1589. CrossRef - Vildagliptin ameliorates renal injury in type 2 diabetic rats by suppressing oxidative stress
Fariba Aghahoseini, Alireza Alihemmati, Leila Hosseini, Reza Badalzadeh
Journal of Diabetes & Metabolic Disorders.2020; 19(2): 701. CrossRef - Small changes in glucose variability induced by low and high glycemic index diets are not associated with changes in β-cell function in adults with pre-diabetes
Kristina M. Utzschneider, Tonya N. Johnson, Kara L. Breymeyer, Lisa Bettcher, Daniel Raftery, Katherine M. Newton, Marian L. Neuhouser
Journal of Diabetes and its Complications.2020; 34(8): 107586. CrossRef - Comparison of the effects of gemigliptin and dapagliflozin on glycaemic variability in type 2 diabetes: A randomized, open‐label, active‐controlled, 12‐week study (STABLE II study)
Soo Heon Kwak, You‐Cheol Hwang, Jong Chul Won, Ji Cheol Bae, Hyun Jin Kim, Sunghwan Suh, Eun Young Lee, Subin Lee, Sang‐Yong Kim, Jae Hyeon Kim
Diabetes, Obesity and Metabolism.2020; 22(2): 173. CrossRef - Glycemic variability: adverse clinical outcomes and how to improve it?
Zheng Zhou, Bao Sun, Shiqiong Huang, Chunsheng Zhu, Meng Bian
Cardiovascular Diabetology.2020;[Epub] CrossRef - Anti-inflammatory properties of antidiabetic drugs: A “promised land” in the COVID-19 era?
Niki Katsiki, Ele Ferrannini
Journal of Diabetes and its Complications.2020; 34(12): 107723. CrossRef - Impact of long-term glucose variability on coronary atherosclerosis progression in patients with type 2 diabetes: a 2.3 year follow-up study
Suhua Li, Xixiang Tang, Yanting Luo, Bingyuan Wu, Zhuoshan Huang, Zexiong Li, Long Peng, Yesheng Ling, Jieming Zhu, Junlin Zhong, Jinlai Liu, Yanming Chen
Cardiovascular Diabetology.2020;[Epub] CrossRef - Visit-to-visit fasting plasma glucose variability is an important risk factor for long-term changes in left cardiac structure and function in patients with type 2 diabetes
Xixiang Tang, Junlin Zhong, Hui Zhang, Yanting Luo, Xing Liu, Long Peng, Yanling Zhang, Xiaoxian Qian, Boxiong Jiang, Jinlai Liu, Suhua Li, Yanming Chen
Cardiovascular Diabetology.2019;[Epub] CrossRef - Effect of dipeptidyl-peptidase-4 inhibitors on C-reactive protein in patients with type 2 diabetes: a systematic review and meta-analysis
Xin Liu, Peng Men, Bo Wang, Gaojun Cai, Zhigang Zhao
Lipids in Health and Disease.2019;[Epub] CrossRef - Efficacy and Safety of Pioglitazone Monotherapy in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials
Fahmida Alam, Md. Asiful Islam, Mafauzy Mohamed, Imran Ahmad, Mohammad Amjad Kamal, Richard Donnelly, Iskandar Idris, Siew Hua Gan
Scientific Reports.2019;[Epub] CrossRef - Effect of DPP-IV Inhibitors on Glycemic Variability in Patients with T2DM: A Systematic Review and Meta-Analysis
Subin Lee, Heeyoung Lee, Yoonhye Kim, EunYoung Kim
Scientific Reports.2019;[Epub] CrossRef - Glycemic Variability: How to Measure and Its Clinical Implication for Type 2 Diabetes
Guillermo E. Umpierrez, Boris P. Kovatchev
The American Journal of the Medical Sciences.2018; 356(6): 518. CrossRef
- What is Glycaemic Variability and which Pharmacological Treatment Options are Effective? A Narrative Review
 First
First Prev
Prev


